No one beats Republicans for hyperbole. And I mean no one. Hyperbole in the right-leaning media makes Joseph Goebbels look “fair and balanced.” Right-wing hyperbole has done more damage to America than the Rosenbergs, child pornography, McCarthyism, and The Bachelor combined.
I kid. But they do tend to get ahead of themselves. And so, of course, when it came to light that military veterans at VA hospitals were put on a secret waiting list for treatments to hide the dire situation from oversight, the right fired up the ol’ hyperbolic comparison engine and got to work, producing ideas like these:
—
Not to spoil the surprise, but Michelle thinks undocumented aliens have a much better time than veterans.
I’ll address both of these momentarily. First, I think it can be debated whether care in the VA is in any degree worse than at conventional hospitals. A recent RAND study showed better-than-average care at VA hospitals. For a variety of chronic and non-chronic conditions, VA patients received the AMA recommended treatments more often than at conventional hospitals. Two studies of patient mortality by the National Institute of Health revealed VA hospitals to be on par with or slightly better than non-VA hospitals. A synthesis of several studies by VA researchers concluded that VA hospitals perform better on process-of-care metrics and equally on risk-adjusted mortality than non-VA hospitals.
Now, I think Michelle and (gulp) Louie Gohmert have a point in that we do a great disservice to our American servicemen and servicewomen in sending them to war all to often. We need to be much more careful in counting the real costs of our wars. I’m proud of our nation for leading the way in treating the mental and emotional scars of war and I hope we continue to resource research and treatment of PTSD and other combat related mental illness.
Come for the employment exploitation; stay for the medical neglect
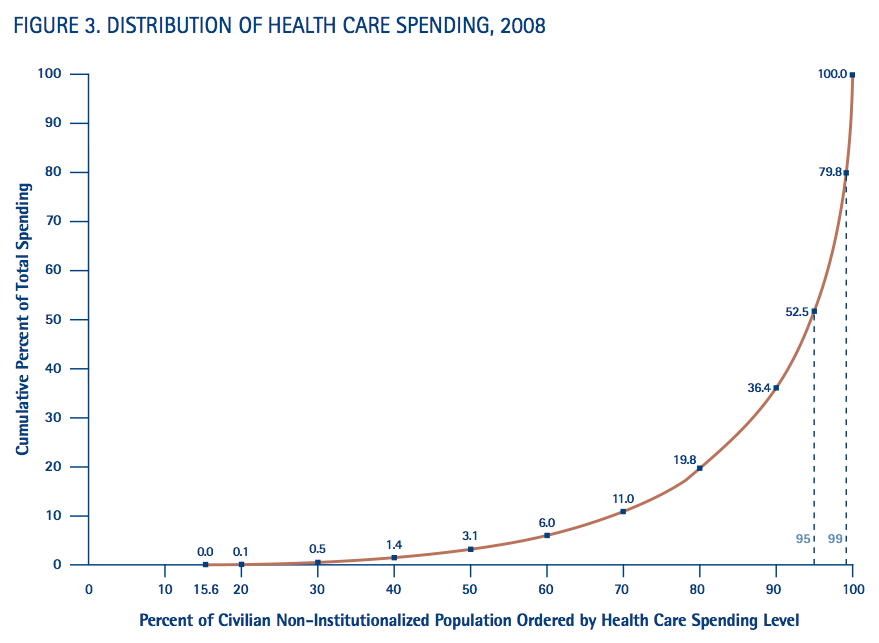
But Michelle, Louie, come on. Before we get to the illegally incarcerated terror suspects, let’s talk about the plight of illegal aliens. They pay taxes but don’t vote or collect Social Security. They are, overall, less likely to commit crimes, but more likely to be the victims of crime. They have little recourse to authorities in disputes with employers and so work in poorer conditions for lower wages. They also use health care resources at a much lower rate. Although immigrants (documented and undocumented) make up 10.7% of the US population, they use just 8% of health care dollars. Of course, immigrants do tend to be younger and therefore healthier, on average, accounting for some of this. But Nadereh Pourat, director of research at the UCLA Center for Health Policy Research, found that illegal immigrants are less likely to go to the doctor, even if they have health insurance for fear of deportation. According to Steve Camarota, director of the moderately anti-immigrant, Center for Immigration Studies, the United States spends about $4 billion per year on health care for illegal immigrants, or about one-fourth of the federal subsidies of crop insurance given to wealthy farmers last year. Since many undocumented immigrants are agricultural laborers, ThisWeekInStupid thinks we should just call that even.
The biggest contributor to poor health care outcomes for undocumented immigrants is that almost half are uninsured. Since they are more likely to be uninsured, health care for immigrants comes more often in free community health clinics and emergency rooms where wait times are much longer and outcomes are significantly worse. Chronic conditions, like the ones that kill most Americans–diabetes, heart disease, etc.–are likely to go completely untreated until problems are very severe. In 2009, Dr. John Z. Ayanian of the National Academies’ Institute of Medicine testified before Congress, summarizing several hundred studies of health outcomes for the uninsured thusly:
Uninsured Americans frequently delay or forgo doctors’ visits, prescription medications, and other effective treatments, even when they have serious disease or life-threatening conditions. … Because uninsured adults seek health care less often than insured adults, they are often unaware of health problems such as high blood pressure, high cholesterol, or early-stage cancer. Uninsured adults are also much less likely to receive vaccinations, cancer screening services such as mammography and colonoscopy, and other effective preventive services.
The result of this lack of access, noted Dr. Ayanian, is that working-age adults are 25% more likely to die prematurely than their insured counterparts.
Now, undocumented immigrants have committed a crime. That’s undeniable. But it’s important to remember that the things they’re doing–working, paying rent in Tuscon, going to the hospital, sending their children to school–are completely legal for you not because you do them differently or because you do less harm or more good than they do, but rather because of where you were born. Some are content to give this fact a “them’s the breaks” shrug and continue on their ungrateful, entitled way. That, in the opinion of ThisWeekInStupid, is quintessentially un-American.
The Posh Life of a Terror Suspect
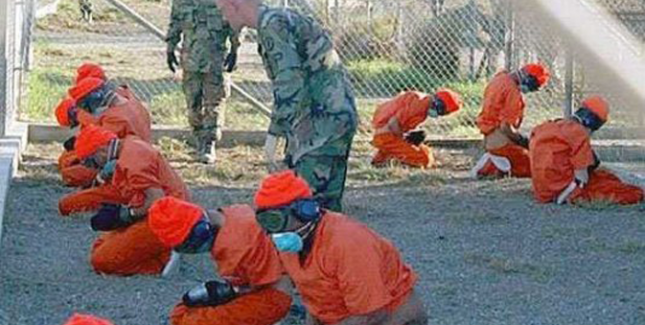
And now for Guantanamo. Picking on Louie Gohmert is no fun. But he was retweeting this story by J.D. Gordon of Fox News. As proof of his claim that we’re nicer to Gitmo terror “suspects” than to veterans, he cited the idea that the ratio of prisoners in Gitmo to physicians is higher than the ratio of veterans to VA physicians in the US. Now, this idea was quickly debunked since the doctors in that tally also treat the soldiers on the base. For many reasons, it’s awfully stupid to declare detainees at Guantanamo Bay have it easy.
Since 2002, 779 men have been detained at Guantanamo Bay. Eight have died. Six were reported by the military as suicides. In comparison with the Phoenix VA, who are currently treating 123,000 patients, that means you are 8 times more likely to die as a healthy 26-year-old sent to Gitmo than as a veteran on a secret waiting list at the Phoenix VA Hospital.
The majority of detainees at Guantanamo Bay have not been charged with any crime. Some are under 18 years old. All are neither judicial prisoners, nor prisoners of war, leaving them with uncertain legal protections. Forty-six prisoners are currently designated for open-ended detention since they are too dangerous for release, but the government has insufficient evidence to try them.
Allegations of torture at Guantanamo Bay, which are many and from varied sources, are difficult to verify. The International Committee of the Red Cross reported in 2004 that prisoners were subjected to humiliating acts, solitary confinement, temperature extremes, stress positions, sleep deprivation and beatings that were “tantamount to torture.” They additionally reported that at least some of the time of these Guantanamo Bay physicians was spent preparing prisoners for “enhanced interrogation” or supervising the same. The New York Times reported the statement of an FBI agent that prisoners at Guantanamo Bay were sometimes left shackled in the fetal position, in their own urine and feces for 18-24 hours. In 2004, an American soldier posing as a prisoner during a training exercise was beaten enough to cause traumatic brain injury and seizures. It turns out even soldiers at Gitmo are treated worse than veterans at the VA.
You’ve probably heard that several dozen inmates at Guantanamo Bay have staged a hunger strike, on-going now for several years. These prisoners have been force fed to keep them alive. Although the video-recordings of force feeding detainees are not available, the actor Mos Def volunteered to be force fed for the camera. I have great respect for Mos Def as an actor, but I think you’ll agree this is legitimately a horrible experience. No one would blame you for not playing the video below, especially if your children are looking over your shoulder.
Take a moment to let this fact sink in: Fox News thinks we should be treating Guantanamo detainees worse.
Now, ThisWeekInStupid is not a pacifist site. We believe a great country often needs defending. But, if there were a nation less than 100 miles from the United States that captured and held young men, charged them with no crime, tortured them and gave no timeline for ever releasing them, wouldn’t our great nation be inclined to intervene? Even at the cost of American lives? I love and revere my nation and am forever grateful for what it’s given me, but I am ashamed we haven’t managed to halt this situation even on our own soil perpetrated by our own soldiers.
So, it’s clear that veterans in Phoenix and likely other hospitals were (and continue to be) treated shamefully, to be sure. But, let’s not lose our heads.